

Print Story
X

So far, ten anti-COVID-19 virus vaccines have been authorised for use in various parts of the world
The Corona virus that has caused the current pandemic is called SARS-CoV-2, or Severe Acute Respiratory Syndrome Corona Virus-2. The disease itself is called COVID-19, or Corona Virus Disease, 2019. So far, ten anti-COVID-19 virus vaccines have been authorised for use in various parts of the world. Eighty one vaccines are undergoing trials with twenty at advanced stages.
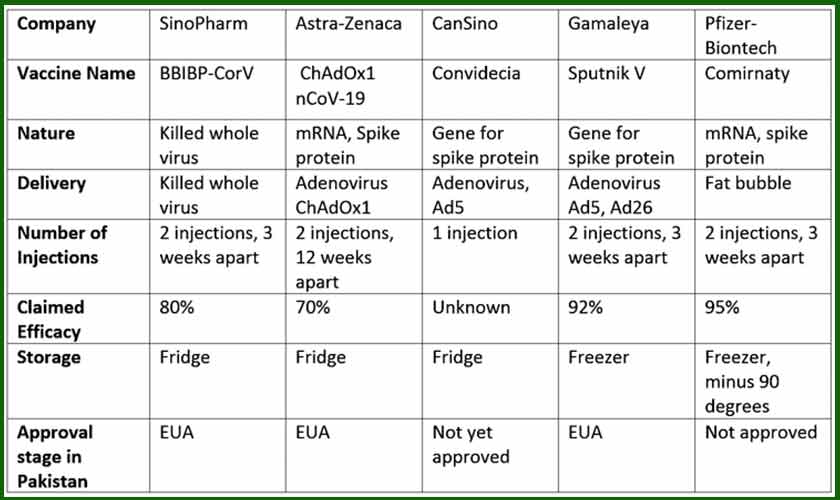
The first one to arrive in Pakistan is a Chinese vaccine made by the state owned Chinese company, Sinopharm. It was developed by the Beijing Institute of Biological Products. It is a whole virus, killed vaccine and has been given an ‘emergency use authorisation’ by the Drug Regulatory Authority of Pakistan (DRAP). The results of the large scale clinical trials, called Phase III trials have not been published yet in peer reviewed medical journals. The trials have taken place in various countries, including UAE and Bahrain. It is thought that the vaccine may be around 80 per cent effective in preventing disease. It is approved for use in adults below 60 years of age. It consists of 2 injections, 3 weeks apart, given in the upper arm.
Many of the vaccines have not been tested in people over 60 years of age. The people of these age groups were told to take precautions and stay indoors. Therefore, the protective effect of the vaccines would not have been easy to determine. However, the likelihood is that they would also get protective immunity from vaccination. This approved use by the competent authorities is allowed when the potential benefits of treatment in public health emergencies are felt to outweigh the risks. A provisional authorisation falls short of a full license. This may be in a situation when the final trials are not complete but the available data shows safety and efficacy.
The second vaccine to be widely used in the country will be the Astra-Zeneca-Oxford vaccine. It was developed by Oxford scientists and manufactured by the Anglo-Swedish company, Astra-Zeneca. This is an mRNA vaccine. It uses another virus as a vehicle to deliver the payload of the CoV2 mRNA to the cells of the vaccinated person. This modified carrier virus is called Chimpanzee Adenovirus Oxford 1, ChAdOx1. This virus cannot divide in humans and therefore is harmless and removed by the body. The mRNA too is like a Snapchat message. It sets the cells off to make and display on their surface, the spike protein which in turn evokes an immune response. The mRNA itself disappears but the body is now pre-warned and prepared for the real deal.
Both of these vaccines can be stored in an ordinary fridge and therefore the logistics are easier to manage, especially the cold chain utilising the facilities of the EPI programme —the Expanded Programme of Immunisation, used for childhood vaccinations in Pakistan.
Another Chinese vaccine called CanSino has completed Phase III trials. The trials included Pakistani patients. The results should be published soon. The likelihood is that it will also be made available to the Pakistani citizens. The delivery mechanism is another Adenovirus, called Ad5, altered in the laboratory to carry the spike protein gene; the protein against which, eventually the body produces immune defence.
The Russians have a respectable record in making vaccines. The Gamaleya Institute in Moscow have made an adenovirus vehicle vaccine, carrying the gene for the full-length spike protein of the CoV2 virus. They have used two different carrier adenoviruses for the 1st and the 2nd dose with the assumption that the immune system will not recognise and fight the carrier virus itself and allow it to deliver the payload to the cells. The efficacy of the current regime is 91%. They are partnering with Astra-Zeneca to trial a combination of their products and see if it works better.
The Pfizer-Biontech vaccine was the first one to be approved in the Western countries. Developed by a husband and wife Turkish couple in Germany, it uses tiny fat bubbles to carry the spike protein mRNA to the cells. It requires a very low temperature of minus 70 to 90 degrees for storage which will make the cost of logistics prohibitive for a country like Pakistan. However rapid technological advances mean that it will soon be possible to store it at temperatures of an ordinary fridge.
The efficacy of a vaccine is the reduction in risk of COVID in people who have received the vaccine, as compared to those who have not. Using this standard, all the vaccines approved for use so far have met the WHO standard of more than 50% efficacy, usually ranging between 70 to 95%. The results so far indicate that the vaccines are pretty safe and the side effects are not significantly more than those of the vaccines which have be around for a long time, such as the Flu vaccine. Most commonly, people can experience injection site pain, aches and pains and mild fever for a day or two. These can easily be treated with paracetamol. Serious reactions are very rare.
Some of the vaccines are using novel mechanisms. The long-term side effects of these vaccines are not thought to be significantly different. However, the scientists will continue to closely monitor the outcomes. According to Faisal Sultan, the Special Advisor on Health, the population coverage that Pakistan is aiming for is about 70 million people. The Economist magazine has projected that widespread vaccine cover would not be achieved in Pakistan before 2023.
The UK vaccination programme seems to have started early and gathered steam quickly. So far, over 11 million people have received at least one dose. Somewhat controversially, the government decided to delay the 2nd dose of the 2 dose regimens, to 12 weeks to achieve a larger population cover. They are also starting a trial of using a different vaccine for the 2nd dose, again to allow flexibility in the vaccination campaign and greater population coverage. If successful, this may be a strategy for Pakistan to consider.
There is a threat of emerging new variants of the virus with evidence that the protective efficacy of vaccines may diminish against some of them. The new technologies, however, would make it possible to tweak the vaccinations to catch up relatively quickly— in a few weeks. This may mean though that periodic booster vaccinations may be needed, such as during winters or when there is a surge.
The writer is a consultant physician in the Queen Elizabeth Hospital, Gateshead, UK. He is the Universal Healthcare Director of KEMCA UK, the King Edward Medical College Alumni Association of the UK. He can be reached at hakimhazik@gmail.com. The recent Universal Healthcare and Education Symposium can be seen at digi-con.net


