

Print Story
X

Choosing therapeutic regimens for the severely sick Covid-19 patients remains a challenge

I
t now looks like a game of chance with unknown odds: lockdown, partial lockdown, no lockdown and a possible return to lockdown.
Meanwhile, we are all holding our breath, waiting and watching as the number of cases rises. For all we know the curve could turn upwards or flatten, even move downwards. For now, Covid-19 is here, and according to the latest statement by the WHO it is not going anywhere very soon.
We need to be prepared and ought to know what to expect over the next few weeks and months. We can have a vague idea of how the pandemic will behave based on what has happened in other countries. A few predictive models have already suggested numbers (of infections and deaths) and dates (of when we are likely to see improvement). However, we also need to be aware of the developments in our understanding of the disease and treatment of Covid-19 patients, even as new evidence is continuously being added to what we know. We have some encouraging new data; we have learnt more about drugs that will not work.
Integrating the experience and results of international trials into routine clinical management of patients requires definite regulatory steps. There are still many unanswered questions related to how best to deliver these treatments. This could mean more research and trials in Pakistan. In addition, a lot will depend on the availability and production of the required drugs in Pakistan.
Predicting the end
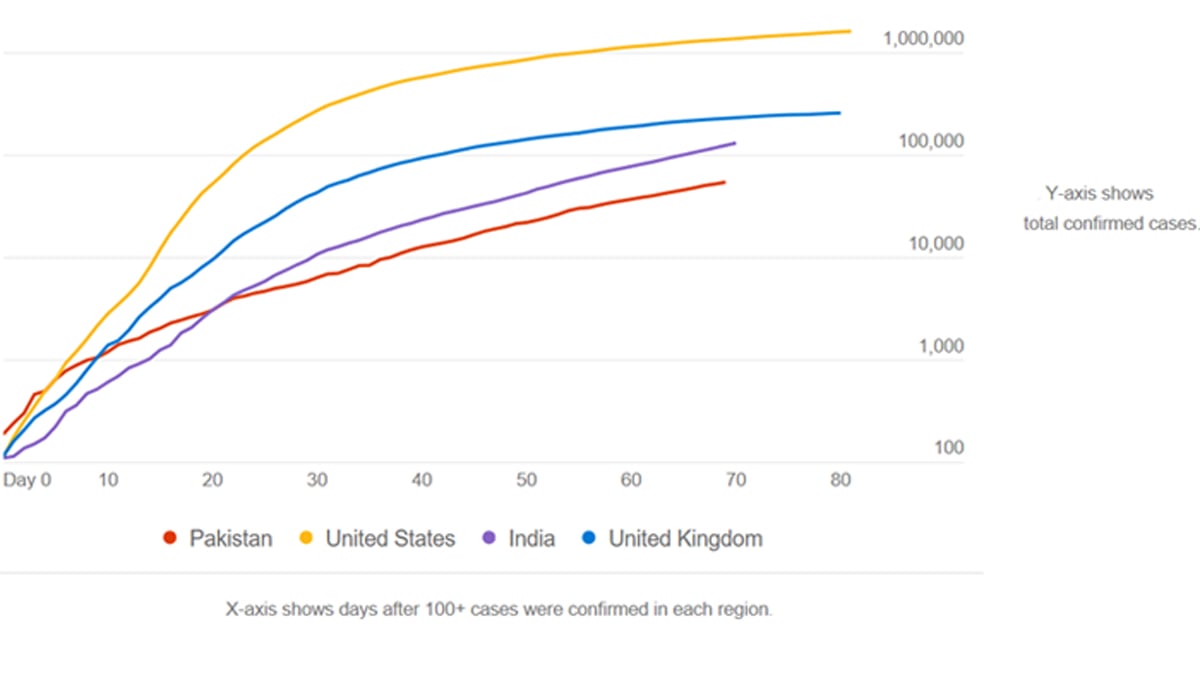
If we review the curves in other countries and compare these to Pakistan’s, there are some notable differences.
The
pandemic in the US and UK spread rapidly within the first few weeks after 100
cases were identified. The factors contributing to the rapid spread are
numerous, but population dynamics and movement are key factors. Initially the
spread of Covid-19 in Pakistan was slow and limited mostly to travellers from
Iran and their contacts. However, this changed within weeks and we saw
community transmission take over. The number of documented cases has been
increasing since then at a steady rate. There are likely several reasons for
this so that the data will require further careful analysis. It could be that
we have more asymptomatic transmission, or that not all symptomatic cases are
being identified. It could also be because of the way the population is
behaving and moving. Most people are apparently not following the prescribed precautions
and the advice to maintain social distance.
The predictive models proposed by Singapore University researchers had suggested that our curve would turn at the end of April and that we would have a 97 percent reduction in the number of new cases by June 9. We have now reached the end of May and our curve is still rising. A few models proposed by Pakistani researchers have predicted that the outbreak will peak between late May and late June and that in the absence of lockdowns it will linger. Accordingly, we have a few more weeks and months of Covid-19 in Pakistan and we need to be able to treat patients.
Update on treatments for Covid-19
Selecting therapeutic regimens for treatment of severely sick Covid-19 patients remains a challenge. The early sources of hope are mostly going out like sparks.
The early hype surrounding hydroxychloroquine as a treatment prompted individuals and nations to stockpile doses leading to a global shortage for the diseases it is meant to treat - malaria and rheumatoid arthritis. Last week, the largest trial of hydroxychloroquine published to date delivered the disappointing news that those treated with the drug had a significantly higher risk of death compared with those who were not. The drug raised the risk of irregular heart rhythm (arrhythmia) that can lead to sudden cardiac death.
Another front runner among treatments being tested is convalescent plasma. A general principle of passive antibody therapy is that it is more effective for prophylaxis than for treatment of disease, therefore investigations are still underway to determine its usefulness. A drawback of this treatment option is that it requires a dedicated set up to collect, process and prepare plasma for clinical use. Accessibility may thus be problematic. We have already seen a shortage of donors in Pakistan, a special call for donations was made a few days ago.
Over the past few months, we have learnt more about the body’s response to Covid-19. This has helped identify additional targets for treatment. One such target is the cytokine IL-6. Two drugs, tocilizumab (Actemra) and sarilumab (Kevzara) that block IL-6 release from our cells, are being tested in phase 3 clinical trials. Published studies have demonstrated that patients who received these inhibitors showed lower levels of inflammatory markers. There were radiological and clinical improvements, and reduced ventilatory support requirements. Researchers are optimistic that an IL-6 inhibitor could be an effective treatment in patients with severe Covid-19. It remains an investigational drug, however, the Punjab Health Department announced that tocilizumab will be prescribed to patients who develop lung complications and who have an abnormal level of IL-6 in the blood.
There is some good news as well. The US National Institute of Allergy and Infectious Diseases has finally published the results of the largest randomised controlled trial using Remdesivir. The study revealed that Remdesivir shortened recovery time of hospitalised patients from 15 days to 11 days. In addition, it showed death in the Remdesivir group was 7.1 percent, compared to 11.9 percent for the placebo group. However, this is not a statistically significant difference. The treatment showed no benefits for severely ill patients on mechanical ventilation – those at highest risk of death.
The investigators highlighted the need to identify Covid-19 cases and start antiviral treatment before the pulmonary disease progresses to require mechanical ventilation. However, given the high mortality despite the use of Remdesivir, treatment with an antiviral drug alone is not likely to be sufficient. Future trials should evaluate antiviral agents in combination with other therapeutic approaches or combinations of antiviral agents to continue to improve patient outcomes in Covid-19. We have no clinical trial data on the efficacy of this drug in Pakistani patients because Remdesivir is so far not available in Pakistan yet.
Price, production and distribution of Remdesivir
Gilead, the company that developed Remdesivir, originally meant it to treat Ebola virus infections. Preclinical data and some clinical studies with other coronaviruses prompted its use in Covid-19 patients. Gilead holds the key to a potential treatment for Covid-19.
The Institute for Clinical and Economic Review, a non-profit organisation that analyses drug pricing, issued an expedited report on Remdesivir. They calculated that if the price is based only on the cost of making the drug, then a 10-day course of Remdesivir should cost about $10. But if the drug is priced based on its effectiveness, ICER estimates it should cost around $4,500 — assuming the drug is proven to have some benefit on mortality. If it only shortens hospital stays, that value-based price goes down to $390. Two other Gilead drugs have drawn scrutiny over pricing in the past. The company charged $1,000 per pill for Sovaldi, a cure for hepatitis C, and its HIV drug Truvada can cost $22,000 per year.
However, Gilead has signed licensing deals with a handful of firms that will distribute generic versions of the drug that will make it more affordable for low- and middle-income countries, including Pakistan. The licence gives the generic companies a right to receive a technology transfer from Gilead for the Remdesivir manufacturing process to scale up production. The companies will be able to set their own prices. In 2015, Gilead provided Ferozsons the license to produce Sovaldi in Pakistan, making it more affordable and accessible for HCV patients in Pakistan.
On May 15, the prime minister’s special assistant on health, Dr Zafar Mirza announced that Pakistan would start “production” of Remdesivir within eight weeks. But production is one thing and universal availability another. Completion of regulatory requirements and import of raw material, testing the first batches then scaling up the production could take several months. Even then the drug will only be available through a clinical trial and under medical supervision as it is still a treatment that is under investigation.
Will Remdesivir be available for clinical use before the end of the pandemic in Pakistan? That question remains to be answered. Only time will tell.


