

Print Story
X

A system of organised blood and organ donations should be created in line with medical morality for better healthcare
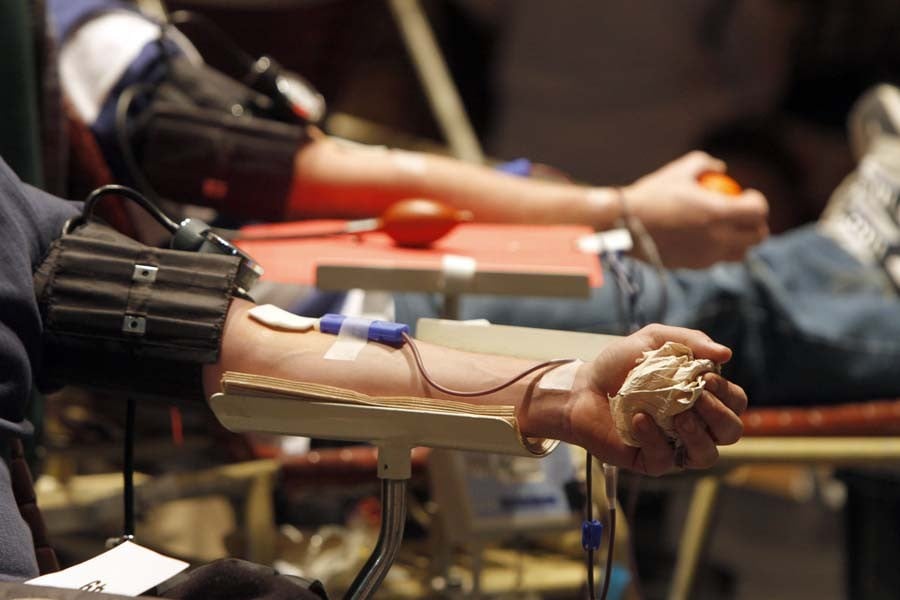
Once every other year or so I write something about transplantation and organ donation. So it will be today. However, in the context of organ donation, I want to include the one type of donation that is extremely important but is rarely emphasised. That is blood donation. One of the great discoveries from more than a century ago was that of blood groups. This led to the development of blood transfusion as a lifesaving method in all sorts of situations.
Major surgery, management of trauma, blood loss during delivery of children, blood replacement in blood diseases were all made possible by the discovery of blood groups and cross matching of blood to prevent ‘transfusion reactions’ which are really nothing but a ‘foreign organ rejection’. Why is all this worth talking about? Simply because blood has to come from a human being and has to be ‘donated’ like any other organ. And even today proper collection, testing, storage and provision of blood donated by volunteer donors are virtually nonexistent in Pakistan.
Almost half a century ago as medical students in King Edward Medical College (KEMC), some of us got together and formed a medical student and young doctor based volunteer blood donor organisation called ‘Anjuman-e-hayat-nau’ that provided blood for patients requiring urgent surgery. The organisation was started by a very dedicated senior medical student named Iqbal Ayub Lodhi who had become junior to us academically because of ‘rustication’ for a number of years after participating in the student strikes in the early sixties. Sadly Lodhi passed away at a relatively young age after graduation.
Most of the blood for surgical patients was and probably still is provided by ‘professional’ blood donors that in those days used to aggregate under a big tree in the lawn across from the Mayo Hospital blood bank. Most of these donors were drug addicts and in the evenings the smell of ‘charas’ (hashish) was quite obvious from that area. The problem was that most families were reluctant to donate blood even for their close relatives so the only source of blood was from these professional donors.
Of course even as medical students fifty years ago we knew that the blood donated by drug addicts could be dangerous to the patient who received it. As a house surgeon in cardiac surgery at that time, I do remember that virtually every patient that received a blood transfusion would get a fever after receiving the blood. I don’t know how much of the present epidemic of Hepatitis B and C in Pakistan is from blood transfusions from these professional blood donors when they switched to injectable drugs a few decades later.
During my time on the faculty of KE a few years ago I found out that students and the young doctors were still donating blood for poor patients in Mayo and affiliated hospitals. But I don’t know if there is a regular organisation that exists to regulate this activity.
Perhaps the Young Doctors Associations (YDA), besides political agitation for their rights, might also want to organise this particular activity at all the major public and private medical colleges, universities and affiliated hospitals. And of course the official blood banks run by the government as well as different tertiary care hospitals should be improved and made sufficiently ‘reliable’ so that volunteer donors can donate blood periodically without worrying that their donated blood will be sold off to the patients that can pay.
In western countries and in the United States where I worked for more than thirty years, besides the major hospitals, the ‘Red Cross’ ran blood banks and blood services all over the country. Most importantly in the US all the donated blood is fractionated and stored as components. The red cells that carry Oxygen are stored as ‘packed’ cells; the plasma is stored separately as are platelets and other components. So if a transfusion is required, it is determined what components are needed and these are then supplied.
During the six years at the department of cardiac surgery in Mayo Hospital I tried desperately to develop the Mayo Hospital blood bank so that it could provide the blood components but interdepartmental politics made it impossible. Till the very end of my time we had to send a person, usually a family member running to the blood centre located on Jail Road to get components made urgently even as the patient was bleeding in Mayo Hospital some five miles away. Yes, that sadly is how public sector medicine works.
I am sure there is an organisation equivalent to the Red Cross in Pakistan called the ‘Red Crescent’ but I have rarely heard or seen it being involved in blood banking services. What the Red Crescent does in Pakistan is at least a mystery to me. Perhaps it is still a viable organisation that just needs some public and government financial support to become active again. And yes I can dream that this organisation can someday function as the Red Cross works in the US.
Coming now to other forms of transplantation and organ donation. Kidney transplantation occurs quite frequently in Pakistan but it is virtually limited to donations by patient relatives or illegally by paid donors. Other forms of donations especially from brain dead patients and recently deceased patients are virtually nonexistent. If these latter types of donations became possible and if paid donations were legalised under strict rules, hundreds if not thousands of lives could be saved. So, I strongly suggest that antiquated sense of morality that prevents many such organ donations be put aside. Saving lives is the basis of medical morality.
For unrelated kidney donors a system of organised donation should be created. A national organisation patterned after United Network for Organ Sharing (UNOS) in the US should be responsible for all un-related donations of organs. All donors that are to be paid should be registered with this organisation and all financial transactions should occur without any contact between the donor and the recipient.
For a kidney donor, I had suggested payment equivalent to the price of a new Toyota Corolla (Toyota Corolla Unit) some twelve years ago. This should also be supplemented by lifetime healthcare for the donor. The cost for all these payments to donors and their families must come through public funds and charitable donations. In this way the criminal transplants that are a danger to both the donor and the recipients will be avoided.
For possible donors that are dying or recently dead, monetary inducements should be made available for the families. Once a pattern of donation of organs of the dying or recently deceased becomes established then unpaid donations might also become more frequent. Eventually laws will be needed that allow automatic harvesting of organs in persons that have agreed to be organ donors.
When I got my US driver’s license I agreed to be an organ donor and this was registered on my driver’s license. Yes that was a long time ago when all of my organs would have been harvestable for transplantation. Now I suppose my ‘corneas’ are probably about the only thing worth donating


