Print Story
X

Lack of information and awareness about the virus, delay in government intervention at the national level, persistent dearth and corruption of funds, and common misperception that HIV only affects ‘people with bad characters’ are some factors affecting the spread and prevalence of HIV/AIDS

Earlier this year when Tanzil Ur Rehman, the programme manager of Dostana Male Health Clinic, walked into his office in Chauburji, Lahore, he realised he wasn’t alone. Four burly strangers had broken in and ransacked his office. Laid out on the table in front of them were condoms and lubricants from Dostana’s supply cabinet. They sat Rehman down to ask why he had such "fahaash" things in his office? They wanted to know "what kind of activities go on in this clinic?"
This was not Rehman’s first brush with violent reactions to his life’s work; he calmly explained that his non-governmental organisation works to promote sexual health awareness, especially about HIV/AIDS, amongst Males having Sex with Males (MSMs) and the gay community, and that the condoms and lubricants on the table are donor-issued and completely legal.
Rehman invited the men to stay a while and observe the clinic. "This technique often works with overly zealous religious men who regard our work distasteful and threaten us. They soon leave out of boredom," he says while sitting in the brightly painted room. The office walls are full of art, from hand-made coasters to amateur oil paintings. The Dostana team keeps their office space colourful and cosy especially since the outside world is hostile to their community and patients. Rehman says neighbours spit on the floor when they see him -- in their eyes Dostana is promoting "immoral, unIslamic and unethical" practices. But, Rehman’s motto is that you can’t stop people from having sex, all you can do is make them have safe sex.
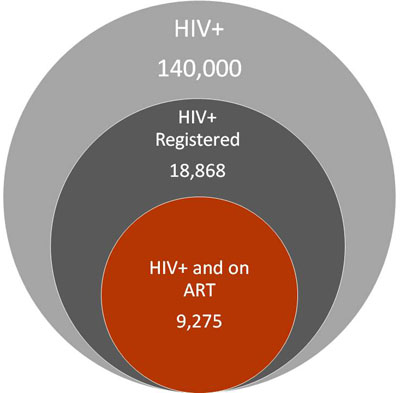
Rehman worries that without genuine government intervention, Pakistan, which is right now experiencing a concentrated epidemic of HIV/AIDS, will soon be facing a generalised epidemic. According to the National AIDS Control Programme (NACP), an organisation dedicated to controlling the spread of HIV/AIDS in Pakistan, there are an estimated 140,000 people with HIV in the country. But NACP officials themselves do not shy away from admitting that the actual number is probably three times as high.
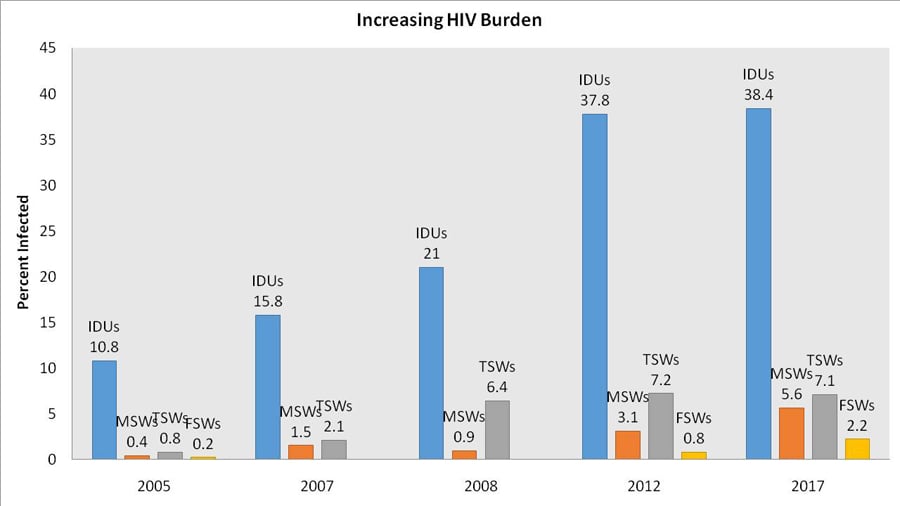
With 20,000 new HIV infections in 2016 alone, Pakistan has one of the fastest growing epidemics in Asia. While the general public has less than 0.1 per cent chance of catching the virus, the chances are exponentially greater for high risk groups. These groups include People Who Inject Drugs (PWID) who have a 38.4 per cent chance of acquiring HIV, MSMs that have a 5.4 per cent chance, and Female, Male and Transgender Sex Workers (MSWs, FSWs, TSWs) who each have a 2.2, 5.6, and 7.1 per cent chance respectively, according to the 2016-17 Integrated Biological and Behavioural Surveillance (IBBS) report -- a round-up of HIV high risk groups conducted by the NACP with help from a Canadian research team.
It is beyond Rehman’s comprehension how the government can’t see that we are following the footsteps of India and Thailand. In both countries the human immunodeficiency virus (HIV) -- a virus that attacks the immune system, the body’s natural defence against illness -- was first spread within high risk groups. Then through bridge populations -- i.e, people who aren’t high risk but regularly interact with high risk groups, such as truck drivers, jail inmates, clients and partners of commercial sex workers -- the virus spreads to the general population.
Rehman explains that containing HIV when it has reached a generalised epidemic level requires much more effort and finances than Pakistan needs right now to contain its concentrated epidemic.
Read also: HIV -- the Sindh chapter
"In the 1970s and ’80s, there was no treatment available for HIV, there was also no electronic and social media that could relay HIV prevention and awareness information to millions of people in seconds," he notes. But today, prevention is easy and treatment is inexpensive: the virus can be, and in other countries is being, contained from spreading, then why is it that in Pakistan HIV prevalence grew at a rate of 17.6 per cent from 2005 to 2015?
***
THE ANSWER CAN BE FOUND in intertwined layers: years of social stigma against HIV, lack of information and awareness about the virus amongst the general population as well as the medical community, the delay in government intervention at the national level, a persistent dearth and corruption of funds, and the common misperception that HIV only affects ‘people with bad characters’ or more scientifically speaking, high risk populations.
Despite the growing HIV/AIDS epidemic, Pakistan is not yet ringing alarm bells because its concentration is found in groups that have historically been marginalised. The figure below shows how HIV prevalence in each high risk group (PWIDs, MSMs, FSWs, MSWs, TSWs) has steadily grown in the last 15 years. This is striking because since 2006 Pakistan has been a recipient of antiretroviral (ARV) therapy. The regular intake of ARV and healthy diet can keep the HIV infection from turning into its more dangerous form of Acquired Immune Deficiency Syndrome (AIDS) for many years, possibly even for a lifetime. The virus destroys a type of white blood cell in the immune system called the CD4 cell. As HIV destroys more CD4 cells, it gradually breaks down a person’s immune system. This means that people with HIV will find it difficult to fight infection and disease -- even a flu or diarrhoea can be fatal.
This is where the ARV medicine comes in. The drug, which is provided to Pakistan absolutely free of cost by The Global Fund, an international financing organisation that aims to fight HIV/AIDS, Tuberculosis and Malaria, keeps the CD4 count from dropping and contains an HIV-infected person’s viral load, which not only allows you to live a healthy, regular life, but also prevents your body fluids from transferring the virus to anyone else.
ARV is basically a miracle drug that has fought many battles -- to be as inexpensive as it is today, at Rs10,000 per year per patient. If an infected person is put on ARV, their likelihood of passing the virus, even through sex, pregnancy and childbirth, is reduced to an almost negligible chance. Unfortunately, out of the meagre 18,868 NACP-registered HIV patients in Pakistan, only 9,275 are under ARV treatment. And even with those numbers, there is no way to ascertain if they are taking medication regularly.
***
TAKING THE MEDICATION EVERY DAY for the rest of your life is no mean feat. Especially difficult is the first month of HIV medication. Last month, while drawing blood from an HIV patient, Rehman of Dostana pricked his finger with a dirty syringe. He understood that this counts as exposure to infected blood and rushed himself to Jinnah Hospital which houses one of Lahore’s four HIV/AIDS treatment centres. He told the doctor on duty about the prick, had himself registered in the clinic and was given a month’s dosage of post-exposure prophylaxis (PEP) -- a drug very similar to ARV that would ensure that Rehman doesn’t catch the virus despite exposure.
But while the medicine is being introduced into your blood stream, it takes a heavy toll on your body. Rehman describes it as a minimum of 30 days of extreme nausea, dizziness and confusion, these side effects can last for up to three months. It’s no wonder then that so many HIV patients take their first month’s dosage from HIV clinics, but don’t return the next month. "HIV is a lifelong disease, which is why it needs lifelong medication, hence counselling is crucial. No one can stay on the medication without proper counselling," says Rehman, whose organisation, Dostana, houses two counsellors.
Dr Servat, who has been counselling HIV patients for many years, now works at Dostana. She describes that since the disease is much more prevalent in the lower socioeconomic classes where awareness and literacy is minimal, a large proportion of patients won’t know what HIV/AIDS is. Those that do, won’t fully comprehend that the virus is lifelong and fatal if left untreated. "Then there is a portion of people who ask that if the medicine won’t cure us, then what’s the point of taking it," she says.
There are also those that are willing to take the medication, but are mentally hounded by the social stigma of HIV. There are even those whose families, upon finding out their HIV status, throw them out or separate their bartan and living spaces. For all these groups, counselling is vital.
Another important element of counselling is to ensure that HIV carriers are careful about containing the virus. "There are some patients, usually teenage boys, who are spiteful about catching HIV," says Rehman. "They then try and spread the disease as a form of revenge."
The virus can be spread by sharing infected needles, through the sexual mode of transmission, the transfusion of infected blood, and from an infected mother to child during pregnancy or birth. But there are a few other ways. "Do you remember in the early 1990s, grapevines were telling Pakistanis to avoid public places because vengeful men with HIV were waiting to cut you with infected blades?" asks Rehman.
Read also: Editorial
The rumours were probably just rumours, but the fact remains that HIV can and has been passed through infected blades.
***
SHOAIB, WHO WORKS AS A RELATIONSHIP MANAGER at a private bank in Karachi, claims to have caught HIV from a dirty blade that pierced him at a barber shop in D.H.A, Karachi.
Shoaib’s* life had always been curated: weekdays were meant for work, Saturdays were devoted to his parents, and Sundays were spent watching mindless television with his two children and gently arguing with his wife. On one particular Sunday in 2015, his daughter asked to be dropped to her friend’s house to prepare for a weekly test. After dropping her, Shoaib spotted a generic-looking barber shop, Cutz and Shavez, in the neighbourhood. He opted to get a shave and haircut in the time his daughter revised her Chemistry concepts.
Little did he know that this would be one of the last professional shaves he ever got. It was near his cheekbone that the barber’s hand slipped. The cut was small but deep. The barber apologetically made a fuss and dressed the wound.
Shoaib collected his daughter and went about his usual Sunday. Six months went by, without event. Then, Shoaib caught a cold that wouldn’t cease. The cold turned into pneumonia and he was admitted to a private hospital whose name he doesn’t wish to disclose. They were able to curtail the pneumonia but Shoaib’s health didn’t fully return. His flu persisted on and off, he experienced curious fatigue and body aches, rashes on his hands and arms, and a wavering fever accompanied with chills.
After an almost week-long period of diarrhoea, Shoaib’s family admitted him again to the same private hospital. On the ninth day at the hospital, a nurse came to his semi-private room and hung a sheet of paper over his bed that said "HIV" in red capital letters. Within the hour, the other two rather ill patients sharing the room with him were moved elsewhere. When the doctor finally appeared, he was wearing latex gloves and a face mask despite the fact that the virus is not airborne nor is it communicable by touching. He curtly informed Shoaib he had been diagnosed with HIV. And then added that since the private hospital does not cater to HIV patients, they should immediately move to Civil Hospital Karachi which does. Within the hour, a weak Shoaib and his wife were shown the door of the private hospital.
If you compare Shoaib to the average Pakistani, he has terrible luck in that he is part of the general population and still caught HIV. But if you compare him to the country’s most common HIV patient, he is terribly fortunate.
Rehman describes the most common HIV-infected person in Pakistan will likely be one who persists hand-to-mouth and struggles to save money to travel to the hospital each month to pick up their HIV medication. On the other hand, one of Shoaib’s uncles is a surgeon with his own modest hospital and many connections in the medical world; as a result of this ARV medication is delivered to Shoaib’s house on a monthly basis. He is lucky his financial and social position has allowed him access to medical and mental health care.
***
IT IS THE SOCIAL AND FINANCIAL VULNERABILITY of high risk groups that causes the government and most NGOs to focus on them. But even then there are so many that slip through the cracks. Bilal*, a daily-wage labourer and drug addict, and his family are one such example. The family lives in Shahdara, an impoverished neighbourhood that lies north of river Ravi near Lahore. Bilal was diagnosed during a volunteer camp set up by New Light Aids Foundation approximately two years ago. After testing positive for HIV, his wife and daughter were screened. The hardly-30-year-old wife, and then five-year-old daughter tested positive.
This was hardly surprising since an HIV positive mother, not on ARV medication, has up to 45 per cent chance of passing the virus to her child, especially if extra care is not taken during childbirth. What was pleasantly shocking was that both females are still healthy and have not displayed symptoms thus far.
After being diagnosed, the family was registered at the Services Hospital Lahore and put on ARV, at least five years too late. Meanwhile, Bilal remained addicted to Avil, a cheap antihistamine that has replaced Heroine in terms of popularity and is typically injected, which means that its consumption requires a syringe.
Bilal says that he uses a new syringe whenever he has a choice, which is rare. "Besides, what’s the point of bothering to find new syringes now? I already have the disease [HIV]," he says. Does he at least properly dispose of his syringes so that he doesn’t spread the virus? In response to my question, Bilal mumbles something about how one shouldn’t run from our predestined fate and the fatality of life. It is implied that his answer is no, since he then changes the topic and complains about the attitude of the staff at Services Hospital’s HIV clinic.
Another way in which PWIDs, like Bilal, are mistreated is that even if they come across some extra money and go to a pharmacy to buy a new syringe or a condom, pharmacists turn them away. "The moment they see a dishevelled person, they won’t sell. They think they are doing an act of huge morality, but actually they are just helping the spread of diseases," says Sarfraz, a Lahore-based HIV outreach who currently works for New Light Aids Control Society. His point is that by refusing to sell clean syringes, the pharmacists aren’t going to stop these men from injecting. As we learnt from Bilal, an addict will simply use a dirty syringe. This is why non-governmental HIV organisations such as Nai Zindagi distribute fresh syringes to addicts, and throw away the used ones.
When Bilal first registered, the family was given a one-month supply of medicine: tablets for the adults and a syrup for their young daughter. This continued for about one-and-a-half years, after which Bilal stopped going to Services Hospital to collect the medicine because the last two times he visited, the doctor in-charge was unavailable forcing Bilal to come back emptyhanded. Each round trip to the hospital costs him about Rs300, he says. "The staff is more hostile than helpful, especially when they find out that I have HIV because I am an PWID," he cites to explain the third reason he stopped going.
The family that persists on a hand-to-mouth basis has been off medication for over six months now; this means that when they get back on medication, because of the gap in their intake, the ARV they will be prescribed will be far more intense and less easily available.
Even that bridge can be crossed once they reach it; in order to get there, however, Bilal must be weaned off Avil and either the government or an NGO would have to ensure that the family is given money for ration and transport on a monthly basis. Statistics suggest that without intervention, the family will not survive another decade. Statistics also show that in 1990 there were 100 children between the ages of 0-14 were reported with HIV and in 2015 this number rose to 2,500. And this is an outdated, modest estimate.
According to the aforementioned IBBS report, PWIDs like Bilal are the most vulnerable high risk group with a 38.4 per cent chance of carrying HIV. In 2005, this number was at a mere 10.8 per cent, but due to a lack of government intervention the number has steadily risen every year. According to the survey, those living in Kasur and Karachi are at higher risk -- to be exact, at 50.8 and 48.7 per cent respectively. It’s important to note that like most HIV-carriers, untreated PWIDs don’t keep the virus to themselves. The survey finds that 62 per cent of PWIDs are sharing dirty needles amongst each other. If that isn’t dangerous enough, PWIDs are an active bridging population: roughly 40 per cent of PWIDs are having unprotected sex with a regular partner.
***
UNFORTUNATELY, THIS IS THE BEST conditions have ever been for Pakistan’s HIV patients.
When Nazir Masih, who contracted HIV from a sex worker in the UAE, was diagnosed and banned from returning to the Middle Eastern country as a migrant worker, he not only battled country-wide stigma and discrimination but also complete medical ignorance. The Pakistani government was aware of Masih’s HIV status but they had no idea what to do with this information.
Ignorance was so rampant that a female doctor in Lahore’s Ittefaq Hospital ‘cured’ Masih from HIV in three months, at the end of which she even awarded him with a HIV-free certificate. Then, he was outed by journalists posing as health inspectors in 1990. His next humiliation was at the hands of the then Secretary of Health, who pressured Masih to wear an HIV tag around his neck when in public. "Additionally, the doctor told all my family members to stay away from me and that they should prepare for me dying at any instant," Masih says to me in his dimly lit office whose walls are filled with honours and awards he has won for battling the stigma against HIV/AIDS through his NGO, New Light Aids Control Society, situated in Green Town, Lahore.
"In those days, the moment I announced my status, people backed away from me as if I was a dirty animal," he says. This was the era when we witnessed the "AIDS la-ilaaj hai, AIDS maut hai" (AIDS is incurable, AIDS is death) advert on PTV. Actor Talat Hussain in his classic rendition of the Grim Reaper equated AIDS to death, while on screen you saw a once-healthy jungle burn to ash. Masih says the nature was meant to represent humanity which the virus burnt to the core.
Throughout this time, Masih says, the government did nothing to support its HIV positive population. ARV was globally discovered in 1984 and made available in neighbouring India by 2003 but did not reach Pakistan until 2006 despite the fact that Masih and others HIV patients had been pleading the government for ARV medication. In 2003, when Masih’s HIV turned to AIDS, his friends and colleagues collected money on their own accord and got a six-month course of ARV medication from India for five people. Things were tough. "I would get one batch of medicines and start worrying about how to procure the next batch," says Masih.
Today, despite his virus having been converted to AIDS, Masih is living a fully functional life. While on a mission to help other HIV patients such as Bilal, Masih nurtures a grievance with the government of Pakistan for mistreating him, for not acknowledging his work in the battle against HIV/AIDS and for the long lag in government intervention.
***
REHMAN DESCRIBES that the lag in government intervention has had a long lasting negative impact. People diagnosed between 1987 and 2006 received nothing from government hospitals except for maltreatment. To date, the NACP and its four provincial subsidiaries are not creating the kind of awareness necessary to inform people that HIV/AIDS is treatable.
In order for Rehman’s or Masih’s organisations to help fund or screen patients like Bilal, the Provincial AIDS Control Programmes (PACP) must sign agreements with the NGOs. "Locally, no one gives religious donations or charity for something as taboo as HIV in the Islamic Republic of Pakistan," says Rehman. While Rehman and Masih have been unsuccessful in collaborating with the Punjab PACP, Moon Ali, a transgender female who heads the Khawaja Sirah Society (KSS) has managed to secure a PC-1 with the government. This means that KSS will now be given funds to spread awareness about HIV/AIDS in the transgender society, along with helping community members get screened and treated.
These funds are coming from provincial health budgets. Following the 18th Amendment and the subsequent devolution in 2011, the Ministry of National Health Services, Regulation and Coordination was devolved to the provinces. Since devolution, PACPs have been formed in Punjab, Sindh, Khyber Pakhtunkhwa and Sindh. One of their goals is to create conditions to achieve the UNAIDS 90-90-90 target which calls for 90 per cent of people living with HIV to know their status, 90 per cent to access antiretroviral treatment and 90 per cent on treatment to have suppressed viral loads by year 2020. Currently, according to the NACP, only nine per cent of PWIDS and six per cent of FSWs have been screened for HIV.
The decision to devolve the Ministry of Health, including various public health programmes including the NACP, has adversely affected the HIV response. Lack of national coordination, data analyses and utilisation at a national level, non-availability of national guidance and monitoring show a strong negative impact on the results of this surveillance round. But despite this and the light smattering of corruption that can be traced in all four PACPs, administratively, things at the provincial level appear better than at the federal level.
Dr Baseer Khan Achakzai the director of NACP, and his 24 employees have not been paid their salaries in 12 months. "The last salary I received was in June 2016," he says. This doesn’t mean that all HIV-related projects are at a standstill. Projects being run by the PACPs and The Global Fund continue to receive their funds, HIV medicines are being provided free of cost, but "federal government employees working for HIV have not received a single penny of our salary from the Health Department in a year," he says.
It’s important to note that expenses for Pakistan’s HIV/AIDS programme are mostly covered by The Global Fund. The federal government has to pay approximately a mere 20 per cent, just enough to cover rent for buildings, staff salaries and power bills. And yet it fails. Achakzai believes that a lot of work needs to be done at the federal level to remove the stigma and discrimination surrounding HIV. Amongst other things, the non-payment shows the lack of commitment the federal government feels towards battling HIV/AIDS.
***
THE PACPs, HOWEVER, ARE MAKING SOME MOVES. In Punjab, the arrival of Dr Adnan Zafar as the head of PACP has caused thousands of truckers and transgender people to be screened for HIV, their office building to be renovated, a new library installed, MOUs signed with research universities and state-of-the-art medical technology to be imported.
And it’s not only Punjab’s PACP that is growing, Balochistan’s PACP is also unrecognisable if you compare it to last year. "In 2016 there was a grand total of zero HIV/AIDS screening centres in Balochistan, today the province has screening centres in 27 out of 30 cities -- the three cities that got left out are Awaran, Kohlu, and Musakhel, because the law-and-order situation there is especially dicey," says Dr Noor Qazi who has been at the helm of Balochistan’s PACP for 17 months.
This is not Qazi’s first stint with public health. Before this, he was the provincial coordinator for the Lady Health Worker Programme and he believes that he has a knack for speaking about public health matters that others don’t want to touch on. "I have become somewhat of a health tableeghi -- I am always talking about women’s health, HIV and sexual practices, and correcting people’s fabricated beliefs about medical science," he says.
Qazi is proud of all that his department has achieved, he says: "When I started this job, people told me that we can’t do wall-chalkings about safety measures for HIV because of social taboos, they also said we can’t hold HIV awareness campaigns in girls’ colleges. But I did both these things and more."
Moreover, the Programme ensures HIV screening tests before every operation. Those that test positive are shifted to the Aids centre in Bolan Medical College Hospital and registered patients receive ARV from one of Balochistan’s two treatment centres, located in Quetta and Turbat.
But Qazi understands there is a long way to go. The fact that the entire province only has two treatment centres from where HIV/AIDS positive patients can obtain ARV is unsatisfactory. Since he does not see the possibility of more treatment centres in the near future, he is investing his energies in registered HIV patients. "To ensure that they come month-after-month to take the monthly stock of medication, we incentivise them with ration packages," he says. But despite this, out of the province’s 750 registered patients only 495 are currently under treatment.
And evidence suggests that the numbers are always growing. Ali Raza Mongol, a paramedic and a social activist based in Quetta, said that in June alone five HIV cases were diagnosed in Quetta’s Benazir Hospital Marriabad. A source in the Health Department, who wishes to remain anonymous, says that most of Quetta’s HIV patients are a result of its proximity with Afghanistan and the inter-provincial travel of its citizens. And in Turbat the virus is brought by deported migrants who used to work in the Gulf until they tested positive.
Dr Chakar Riaz, the man in charge of containing HIV in Balochistan before Dr Qazi took over, says that although working with PWIDs, MSMs, FSWs and TSWs is important, the PACP should also look towards truck drivers and mine workers, since both lots of men are away from home for elongated periods of time. "Due to the inter-provincial travel of truck drivers and mine workers, AIDS can never be fully controlled in provincial boundaries," claims Riaz.
Another group to worry about is prison inmates. Last year 26 HIV-positive prisoners were diagnosed in Gadani Jail alone, says Dr Qazi. He also worries about coal miners and drug addicts who refuse treatment. "If someone is not willing to take the treatment, then what are we to do," asks a beleaguered Dr Qazi as he hurries from an HIV presentation at the Secretariat to an HIV awareness talk in a Boy’s High School in Quetta.
***
AWARENESS, OR LACK THEREOF, about HIV/AIDS is a global problem. But in Pakistan, aid workers such as Rehman and doctors suggest that the problem is magnified because of the extreme taboo of the disease and its relation with sex. He cites that awareness is necessary at two levels. The first is at the state level. The government must intervene to ensure the medical community is rid of biases against HIV/AIDS.
While reporting for this story, a family care specialist who works at the Government Nawaz Sharif Hospital near Yakki Gate in Lahore told me to "stay away from HIV specialist doctors since the disease is contagious." A nurse at the HIV clinic in Mayo Hospital says "it’s unlikely that we will curb HIV soon because HIV is a sign of bad character and bad seeds are everywhere." An HIV patient undergoing treatment at Jinnah Hospital says "doctors often treat HIV as a punishment for bad behaviour, instead of a disease."
Needless to say, much work needs to be done in improving the medical community’s attitude towards the virus. A doctor who teaches Community Medicine at King Edward Medical College Lahore explains that the discrimination against HIV is rooted in our education system. "Most teachers skim over the HIV/AIDS chapter as fast as they can, because the moment the class starts, male students, many of whom have already formed incorrect associations with HIV and sex, begin hooting," says the doctor who wishes to remain anonymous. While the textbook themselves are not discriminatory, she points out the medical instructor’s attitude may be. "If we ourselves are not silencing these doctors-to-be from hooting at the very mention of HIV, and we are skimming over the chapter as if the very information it entails is something to be ashamed of, what message about HIV/AIDS are students supposed to derive," she asks.
If this is the situation of Punjab’s most acclaimed medical college, one dreads to think about the situation in smaller cities and smaller colleges. Dr Faryal Waheed, who teaches Community Medicine at Quaid-e-Azam Medical College in Bahawalpur, describes the situation as "bleak". She says that the class on HIV is typically less than half the length of a class on other viruses, because the "nature of the disease is sensitive and most students are snickering and giggling, rather than concentrating".
In fact, most pre-medical students have already built narratives about HIV before even reaching college. "Most students thought of it [HIV] as something that is dirty and mostly related to prostitutes," says Alina Abbas, a former pre-med student who then turned to the arts.
***
THE SECOND LEVEL AT WHICH AWARENESS MUST BE INCREASED is at the level of AIDS activism. "Community members, outreach workers, patients -- everyone needs to do work at the ground level. We can’t just expect the state to do it all," says Tanzil Ur Rehman of Dostana.
But this is easier said than done. With the stakes of ostracisation so high, who would want to work for this cause? Masih does and his work has never been appreciated. Rehman does and he is appreciated by men ransacking his office.
However, there is hope yet. Ahmed Gul*, a resident of Chitral who caught the virus in 2014 in the UAE, paradoxically describes himself as an ‘undercover AIDS activist’.
When Gul was deported to Pakistan, the authorities were aware that he had HIV and he was registered at the treatment centre in Kohat. But KP’s PACP was not functioning seamlessly. Gul could not be treated in Kohat. "Imagine learning that you have a disease that can kill you if left untreated, then add to that the social stigma of HIV, and then picture being told that the government facility you have been registered at is unable to help you, and you will begin to understand why I repeatedly considered killing myself," says Gul.
An official at KP’s PACP, who wishes to remain anonymous, explains that from 2014 to 2016 the PC-1, an agreement which would allow The Global Fund to release medical and financial help for KP, remained unapproved by the provincial government. The financial burden then fell on the Health Department, which failed to rise to the occasion. Treatment and screening centres across the province were shut down and the only facility in the province that continued to screen and treat HIV was the family care centre at Hayatabad Medical Complex which understandably grew financially weaker over the years.
It must be mentioned here that while the entire country exigently needs more HIV/AIDS treatment centres, nowhere is the need more crucial than in KP and the Federally Administered Tribal Areas (Fata). Recently, NewsLens Pakistan, an online news cooperative, reported on the complete lack of HIV/AIDS treatment centres in all of Fata’s seven agencies. The feature cites a story about one Kulsoom Bibi, an AIDS widow, who couldn’t travel the 250 kilometres from Parachinar to Peshawar on a regular basis, and so was forced to rent a residence in Peshawar for her HIV-positive self and her five children.
Eventually, after a two-year gap, in June 2016, the PC-1 was approved, funds were released and five centres that catered to HIV patients were opened. But by then the damage had been done. Out of the estimated 20,000 HIV/AIDS patients in KP, only 2,450 are registered, and even out of these only 1,450 are receiving treatments. "I realised the importance of ARV medication, but other HIV patients didn’t focus on treatment and carelessly spread the disease," says Gul.
He claims that migrant labourers are not taught about the dangers of unprotected sex before they board their flight to the UAE and that is a big cause behind the HIV epidemic in KP. Gul describes how there is a lack of outspoken and dedicated HIV activists in the province.
"Look at me, I want to help and prevent my countrymen from getting this disease, but I am still too scared to raise awareness on a public level because KP is not yet ready to discuss things as taboo as HIV, drugs, and safe sex," he tells me, over the phone. He also does not know of any HIV activists in the province who he can take inspiration from.
***
BACK IN LAHORE, HIV activists and outreach workers are hard at work. About 20 minutes after sunset, Bagh-e-Jinnah, more commonly known as Lawrence Gardens, has fewer visitors than one would expect. Some parts of the park are better lit than others. These areas have groups of men and families lying about enjoying the relief of wind in the middle of the Lahori summer. But I am told that if I’m searching for the spread of HIV/AIDs, I need to move towards the darker areas of the gardens.
It’s in the shadows that MSMs and MSWs find partners and clients. "First we cruise, meaning we walk around the park sizing people up, trying to gauge who we could interest," says Shahid, an MSW who also works as an outreach worker for more than one male sexual health organisations. Many NGOs hire outreach workers who are former, or at times current, sex workers or former drug users. This makes it easier for sex workers and drug users to trust the NGO workers. Shahid visits Lawrence Gardens daily, sometimes he makes some money and sometimes he just makes a new friend. But every day he tries to educate people about the importance of condoms.
Carrying condoms is dangerous in Pakistan, especially for sex workers. "For the police, it’s proof that you were about to commit an unlawful act," says Ferzana, a former female sex worker. She describes that when out on the streets of Karachi, if stopped by the police, the first thing she would do is drop the condoms she had been carrying. "For the police, condoms were evidence to lock us up until our caretaker would come and bail us out," she says.
The irony is stark; the one item that can effectively and efficiently protect her from HIV and other STDs is itself considered illegal. However, she also adds that clients that deemed to wear condoms were few and far between.
Shahid agrees. He says that the clinics he works for instruct him to distribute condoms to MSWs and MSMs, but the prevalence of condom-use is strikingly low. "Almost no one uses them. Often I find them lying unopened in the trash bin the next day." Even sex workers who understand that condoms are the most effective and cheapest prevention against HIV are pushed into a corner. "If the client does not want to use one, there’s literally nothing the worker can do," says Shahid.
The lack of condom usage that can be observed in Lawrence Gardens is well represented in country-wide statistics. In the most recent IBBS survey, only 8.6 per cent of MSWs and 8.3 per cent of MSMs regularly used condoms. The survey further revealed that 5.6 per cent of all MSMs are HIV positive. Add to this the fact that on average MSWs and MSMs reported having from two to six sexual partners a month, and that 22 per cent of MSWs and 37 per cent of MSMs are married and presumably are having regular sex with their wives, and you will begin to understand the spread of the disease.
While walking with Shahid through the park, we were stopped several times. Different people wanted different things. One man, who works as a business developer at an architecture firm and visits Lawrence, weekly wanted to inquire if Shahid could set up a discreet HIV testing appointment for him on a Sunday, he also asked if Shahid had some condoms on him to spare? Another man had been really unwell and wanted to know if screening tests were free? The aforementioned survey reveals that only 34.9 per cent of MSMs are aware of HIV prevention programmes in their city, and of these only 13.3 per cent avail services from either the government or NGOs.
The last group that approached Shahid was not from the shadows. The group of six men were from the well-lit park where the children were playing. They wanted to know if Shahid or any of his male accompaniments were up for business, hence displaying that it only takes a few minutes for HIV-spreading bridges to form between MSWs and the general population.
***
THERE ARE MANY OTHER SUCH NETWORK INTERACTIONS, explains Rehman. The IBBS survey finds that a large proportion of truckers are interacting with TSWs, almost 36 per cent of PWIDs are having sex with FSWs, and almost 29 per cent are meeting MSWs or TSWs. And as mentioned before, a large number of infected truckers, SWs, and PWIDs are regularly having unprotected sex with their partners.
The numbers keep increasing and, according to NACP’s Dr Achakzai, Pakistan has the second largest HIV positive population in South Asia. He reiterates that the number of patients registered in Pakistan is too modest and that the missing population are "silent killers" who are spreading HIV. "Registration and treatment must increase, and taboos must decrease," says Rehman. "Currently we are a country where carrying condoms is more dangerous than guns, and in order to inverse that, the people, the patients, the media and the government must talk more openly about sex, drugs and HIV."
*Names have been changed to protect privacy.
Reporting contributed by Adnan Aamir from Quetta and Waqar Gillani from Islamabad